A Randomized Trial to Reduce Inappropriate Prescribing to Older Adults Visiting the Emergency Department
GEMS-Rx Guidelines: 2024 Geriatric Emergency Medication Safety Recommendations (GEMS-Rx) identify 8 medication classes that are high risk (i.e., not recommended) for older adult (65+) patients.
Frequently Asked Questions (FAQs)
Which medications are considered potentially inappropriate?
The 2024 GEMS-Rx recommendations identify eight high-risk medication classes for older adults (65+): barbiturates, benzodiazepines, first-generation antihistamines, metoclopramide, first-generation antipsychotics, nonbenzodiazepine hypnotics (Z-drugs), skeletal muscle relaxants, and sulfonylureas. These are considered potentially inappropriate when safer alternatives exist.
How soon will I see a change in my performance report after adjusting my prescribing?
Reports are generated from the most recent 90 days of prescribing data, so sustained changes may take a few weeks to appear. Continued adherence to GEMS-Rx recommendations will be reflected in subsequent feedback cycles. Rx recommendations will be reflected in subsequent feedback cycles.
How are prescriptions attributed?
The attending clinician listed on the patient’s discharge is recorded as the prescriber. When trainees write or enter orders, the supervising attending on record is considered the responsible prescriber for reporting purposes.
Medication orders may be entered by trainees or supervised APPs during the visit; however, prescribing outcomes are attributed to the attending physician responsible for the patient at discharge, consistent with standard ED quality reporting practices.
For encounters in which an APP cares for a patient independently (i.e., without an attending physician assigned), the prescription will be assigned to the APP.
How are prescriptions assigned to a prescriber?
The attending clinician listed on the patient’s discharge is recorded as the prescriber. When trainees write or enter orders, the supervising attending on record is considered the responsible prescriber for reporting purposes.
Medication orders may be entered by trainees or supervised APPs during the visit; however, prescribing outcomes are attributed to the attending physician responsible for the patient at discharge, consistent with standard ED quality reporting practices.
For encounters in which an APP cares for a patient independently (i.e., without an attending physician assigned), the prescription will be assigned to the APP.
How are clinicians assigned to facility groups?
Please follow these steps to view your GEMS‑Rx performance report:
- Log in to Epic
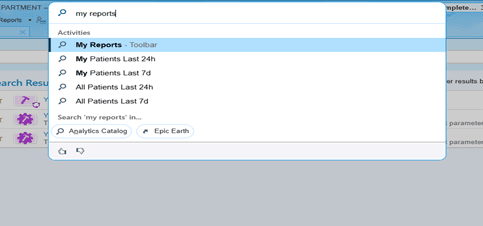
- Click “My Reports” in the toolbar at the top. Alternatively, you can use the universal search and type “My Reports”:

- In the Analytics Catalog search bar (in the ribbon below the first one), search for “GEMS” and press enter:
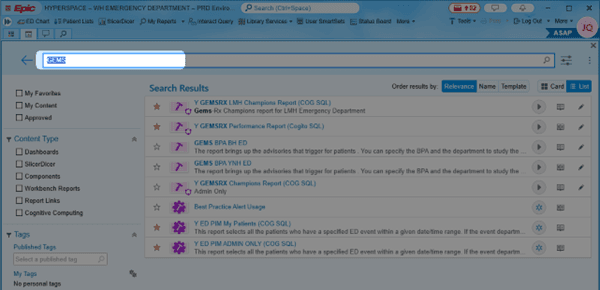
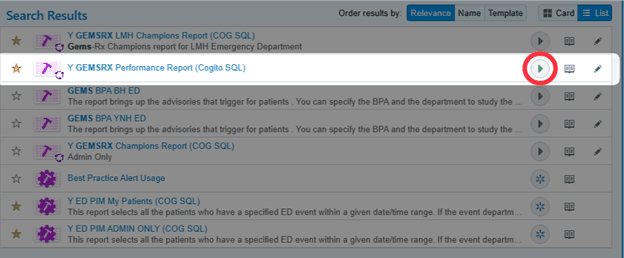
- Find the report titled “Y GEMSRX Performance Report (Cogito SQL)”, double click the report or click the green play to the right to run the report.
Note:If you are the clinical champion, select the report titled “Y GEMSRX Champions Report (COG SQL)”; you must have privileges to run this specific report.
How do I opt out of receiving messages?
Participation is voluntary. If you choose not to participate or later wish to withdraw, you will not receive any further messages. If you wish to stop receiving messages, please contact Jennifer.arango@yale.edu to unsubscribe. Once withdrawn, you will not be able to rejoin the study later.